Teaching Module
TRIANGULAR CORD SIGN OF BILIARY ATRESIA
Contributed by :Dr Kalpesh Khatal, DMRD
Dr Anirudh Badade
In neonatal cholestasis, it is important to differentiate biliary atresia from neonatal hepatitis as a cause of the jaundice.
Early diagnosis of biliary atresia is important for achieving a favorable outcome. If the Kasai operation is performed within the first 2 months of life, more than 60% of infants will achieve jaundice-free survival [1]
A positive triangular cord sign is hallmark of the biliary atresia.
Triangular cord sign is a thick tubular or triangular echogenic density (fibrous ductal remnant) along the anterior aspect of the portal vein at its bifurcation into the right and left branches.
Absence of triangular cord sign (normal) : 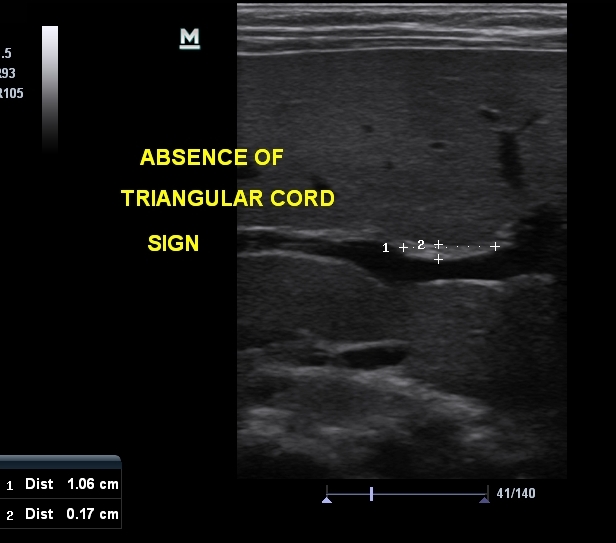

Presence of triangular cord sign
Positive of triangular cord sign = thickness of EARPV > 4 mm on a longitudinal scan
(EARPV - echogenic anterior wall of the right portal vein)
Use of a 4-mm thickness as a criterion for diagnosis of biliary atresia has been reported to have sensitivity of 80% , specificity of 98% , a positive predictive value of 94% , a negative predictive value of 94% , and accuracy of 94% .
What is the anatomic correlate of the triangular cord sign ?
Biliary atresia is characterized by fibrous obliteration of extrahepatic bile duct with fibrous ductal remnant in the porta hepatis. The hepatic duct transform in to a fibrous ductal remnant that is usually anterior and slightly cranial to hepatic artery and the portal vein. The fibrous ductal remnant takes course as the common hepatic duct and smoothly tapes proximally along the both sides of the intrahepatic duct. Thus, the location of the fibrous ductal remnant in the porta hepatis should be the same as that of common hepatic duct.
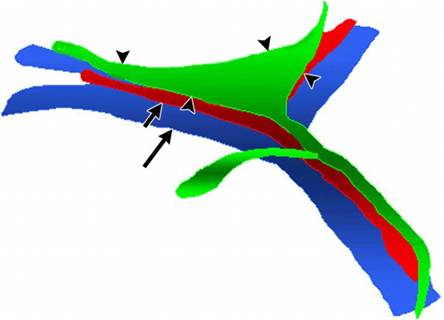
Schematic drawing represents the anatomic relationship between the fibrous ductal remnant and blood vessels around the porta hepatis. The triangular, cone-shaped, fibrous ductal remnant (black arrowheads, green) is positioned anterior and slightly superior to the portal vein (long arrow, blue) and the hepatic artery (short arrow, red).
http://radiology.rsna.org/content/229/2/395/F2.expansion.html
References
1. Ohi R. Biliary atresia. In: Balistreri WF, Ohi R, Todani T, Tuscida Y, eds. Hepatobiliary pancreatic and splenic disease in children, 1st ed. Amsterdam: Elsevier, 1997:231 -260
2. Abramson SJ, Treves S, Teele RL. The infant with possible biliary atresia: evaluation by ultrasound and nuclear medicine. Pediatr Radiol 1982;12:1 -5 CrossRef Medline
3. Kirks DR, Coleman RE, Filston HC, Rosenberg ER, Merten DF. An imaging approach to persistent neonatal jaundice. AJR1984 ;142:461 -465
4. Kotb MA,Kotb A, sheba MF, Et al. Evaluation of triangular cord sign in the diagnosis of biliary atresia. Pediatric 2001;108;416-20
5. Brun P, Gauthier F, Baucher D, et al. ultrasound finding in biliary atresia in children. Ann Radiol 1985;28:259