Case Reports
Case 5 : Syrinomyelia
Scripted by : Dr Kalpesh KhatalEdited by : Dr Sangeeta Jain, MD, Vridhi Fertility Centre, Vardhaman hospital, Ambala City
Contributed by : Dr Anirudh Badade
Abstract :
Sirenomelia or Mermaid syndrome represents severe form of caudal regression.It is a rare congenital malformation that is incompatible with life. In the following case report, we encountered with Sirenomelia at 15 wks of gestation in 23 year old female , who was scanned for the first time at our centre.
Introduction:
The Sirenomelia resembles the mermaid of Greek & Roman mythology , which means head & upper body of a human and tail of a fish. It is a severe form of caudal regression syndrome that results in fusion of lower extremeties,which is not compatible with life. A spectrum of anomalies affects primarily the musculoskeletal, genitourinary & gastrointestinal systems in this syndrome.This rare syndrome has a reported incidence of approximately 1 in 60,000 to 1,00,000 births with a range of 0.1 to 1 % of all malformed infants.There are approximately 300 cases reported in literature so far , 15 % of which are associated with twinning, most often monozygotic. This syndrome has strong association with maternal diabetes where relative risk is 1:200 - 250 & upto 22 % of these fetuses with this anomaly will have diabetic mothers.First medical description of Sirenomelia was by Rocheus & Polfyr way back in 16th century.Duhamel in 1961 defined all the anomalies of mermaid syndrome & described it most severe form of caudal regression syndrome.
Case report:
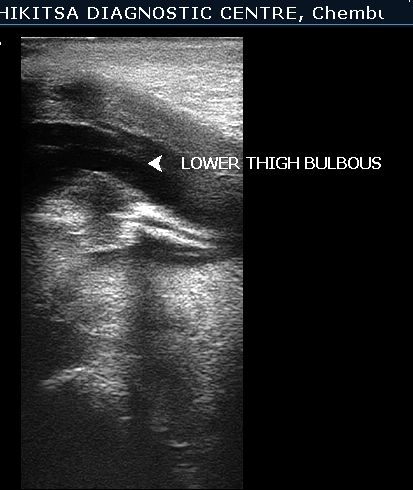
A 23 year old Primigravida was scanned at 15 weeks gestation for the first time. On U/S - she was having severe oligohydramnios. The lower limbs of fetus were found to be fused & proximal portion contained 2 long bones ( Femora ). External genitalia of fetus were not visualised. On colour flow , the fetus was found to have single umbilical artery. Other congenital anomalies could not be ruled out because of severe oligohydramnios & period of gestation at which ultrasound was performed. The patient was referred back to the obstetrician for further management.In view of congenital malformation incompatible with life , MTP was carried out by obstetrician & diagnosis was confirmed.

DISCUSSION :-
A congenital anomaly, caused by a disruptive vascular defect, characterized by fusion of the lower extremities. It is a very rare congenital deformity in which the legs are fused together, giving them the appearance of a mermaid's tail.
This condition is found in approximately one out of every 100,000 live births, with a male to female ratio of 3:1.
The fusion of the lower limb has been classified into three types:
1) Apus- no feet, only one tibia and one femur,
2) Unipus- one foot, two femora, two tibiae, two fibulae,
3) Dipus- two feet and two fused legs (giving the appearance of a flipper).
This latter type is also called "mermaid syndrome".
This pattern of birth defects is associated with abnormal umbilical cord blood vessels. The normal fetus develops two umbilical arteries, which pump blood from the fetus to the placenta, and one umbilical vein, which returns blood from the placenta to the fetus. The umbilical arteries branch off the iliac arteries in the pelvis. The iliac arteries supply the legs and pelvic organs such as the genitalia.
Most babies with sirenomelia have only one umbilical artery and one vein. Rarely a baby with sirenomelia can have the typical two arteries and one vein with occlusion (blockage) of one artery.
In sirenomelia, the one functional artery is larger than normal and branches from the aorta high in the abdomen. Below this umbilical artery, the aorta becomes abnormally narrow. This type of single umbilical artery is known as a vitelline artery because it is thought to arise from the primitive vitelline arteries early in the life of the embryo. The vitelline arteries normally fuse a few weeks after conception to form the arteries that supply the gastrointestinal system and genitourinary system (superior mesenteric, inferior mesenteric, and celiac arteries).
If the normal umbilical arteries do not form correctly as branches from the iliac arteries, then a vitelline artery might persist.
The vitelline umbilical artery steals blood and nutrition from the lower body and diverts it to the placenta.
This results in a small aorta and variable absence of the arteries that supply the kidneys, large intestine, and genitalia (renal, inferior mesenteric, and celiac arteries). Because of the loss of nutrition and blood flow, the lower limbs fail to form as separate limbs, the kidneys do not form or are malformed, the large intestine ends blindly in the abdominal cavity, the anus is imperforate, and the internal and external genitalia are absent or malformed.
Sirenomelia has been reported as a result of teratogenic agents .
A teratogenic event during the gastrulation stage i.e. 3rd gestational week, may interfere with the formation of notochord, resulting in abnormal development of caudal structures.1,5 Altered oxidative metabolism from maternal diabetes may cause increased production of free oxygen radicals in the developing embryo, which may be teratogenic.
9 Hibelink et al. have demonstrated that an intravenous administration of cadmium and lead can produce sirenomelia in the golden hamster VonLennep et al.8 described a case of partial sirenomelia and discussed a possible teratogenic effect of vitamin A.
Three pathogenic theories have been proposed to explain this malformation,including:
1) a pressure theory
2) primary failure in the development of caudal somities that leads to defective development of the lower parts of the embryo and
3) a lack of nutritional support to the caudal region of the body"s embryo.
Some authors consider this anomaly as one of the clinical manifestations of the “caudal regression syndrome” that is a consequence of an abnormal development of structures derived from the caudal mesodermal axis of the embryo before the fourth week of gestation, and extended to various craniocaudal levels.
This leads to an absence of genitalia (except for gonads) and renal agenesis when paramesonephric and mesonephric ducts are involved. According to Barr, if the mesonephric ducts progress enough to reach the ureteric buds and penetrate the metanephric blastema, the kidneys can be formed. Sometimes the metanephric part of the intermediate mesoderm is damaged or defective; in this case, hypoplastic or abnormal kidneys may be present such as in our case.
Anomalies associated with sirenomelia in order of frequency are: Facial anomalies (Potter, face), single umbilical artery (usually the right), imperforate anus, genitourinary system agenesis, no external genitalia or ambiguity, lower sacral/vertebral defects, cardiac anomalies, abdominal wall defects, malformed thorax, and usually severe oligo- or anhydramnios.
When unexplained oligo-anhydramnios is observed in the second trimester of pregnancy, in the absence of PROM, the diagnosis of sirenomelia can be considered together with the other main causes such as Potter"s syndrome, Meckel-Gruber syndrome, polycystic kidneys, obstructive uropathies and severe IUGR.
The differential diagnosis may be difficult when a "mermaid syndrome" (the most rare) with cystic kidneys is present. Because oligo-anhydramnios is almost always present, the injection of saline solution in the amniotic cavity may improve the visualization of the fetal anatomy. Sirenomelia is differentiated from these conditions by the anomaly of the leg: reduced numbers of long bones, abnormal proximity of the femurs, and absence of motion of the legs
Acknowledgment:- We take immense pleasure in thanking Dr.Anirudh Badade for his able guidance and useful suggestions.
References
1) Kallen, B; Castilla, E E; Lancaster, P A; Mutchinick, O; Knudsen, L B; Martinez-Frias, M L; Mastroiacovo,P; Robert, E (1992). "The cyclops and the mermaid: An epidemiological study of two types of rare malformation". Journal of Medical Genetics 29 (1): 30-5.
2) Van Keirsblick J, Cannie M, Robrechts C, de Ravel T, Dymarkowski S, Va den Bosch T, et al. First trimester diagnosis of Sirenomelia. Prenat Diagn 2006; 26: 684-8.
3) Akbayir O, Gundorduk K, Sudolmus S, Gulkilik A, Ark C. First trimester diagnosis of Sirenomelia: a case report and review of the literature. Arch Gynecol Obstet 2008; 278: 589-92.
4) .Valenzano M, Paoletti R, Rossi A, Farinini D, Garlaschi G, Fwcheri E, et al. Sirenomelia. Pathological features, antenatal ultrasound clues and a review of current embryogenic theories. Hum Reprod Update 1999; 5: 82-6.
5) Baxi L, Warren W, Collins MH, Timor-Tritsch IE. Early detection of caudal regression syndrome with transvaginal scanning. Obstet Gynecol 1990; 75: 48